
A 62 years old man
Weight: 97kg
Height: 175cm BMI: 31.7 kg/cm2
Type 2 diabetes (HbA1c: 63 mmol/mol) (7,9)
Duration of diabetes: 12 years
Smoker of 5 cigarettes/day
Hypertension, hypercholesterolemia
Proliferative diabetic retinopathy and loss of vision
Living alone
The ulcer was noted by a district nurse during routine examination.
When asked, the patient explained that although he knew he had a wound for 3 weeks, he did not seek any medical advice as he had no pain and he did not consider that the wound was severe.
- To provide an interactive case scenario that takes the clinician through an example of a non-complicated DFU
- To reinforce the need for holistic assessment of the patient
- To reinforce the need for incorporating the principles of standards of care in the management of DFU
- To reinforce the need for early referral to the specialist foot service team or to the Multidisciplinary Foot Team
What factors from patient history would make you concerned?
Correct answer :
yes: The patient is likely to have neuropathy as he did not feel any pain and he could not explain how the ulcer developed
Correct answer :
yes: Having loss of vision means that he is at high risk for developing recurrent foot ulcers and will need more intense follow up in the care plan.
Correct answer :
yes: This patient has additional cumulative risk factors: smoking, hypertension, poor diabetes control & dyslipidemia, indicating that his risk for peripheral arterial disease is high.
What factors from patient examination would make you concerned?
Correct answer :
No: less urgency
(have a link to ISDF classification)
Correct answer :
No: This indicates a negative “probe to bone” test hence the infection has probably not spread to the bone and the ulcer appears not complicated
(have a link to video on probe to bone test)
Correct answer :
True: In this case at first glance, we can assume that peripheral arterial disease will not be that prominent, and the presence of fast healing time on follow up will confirm this hypothesis.
Correct answer :
False: the clinician is urged to inspect both feet and shoes (including the in-house and outdoor shoes). 85% of all DFUs are related to un-adapted shoes. In this case the shoes had an artifact at the site of the ulcer.
What factors from patient history would make you concerned?
Correct answer :
Yes: it can be an indicator of non – compliance and denial
Correct answer :
Yes: Looking at the profile of the patient and especially knowing that he has loss of vision, social follow up should be considered for an improved outcome.
Correct answer :
YES: Checking the status of tetanus vaccination and allergies is important for those patients. Most of the patients are not vaccinated for a long period of time.
What investigations would you undertake during the patient’s visit?
Correct answer :
yes: a careful assessment of the wound characteristics is important: no odour, no increased temperature, no exudation, depth not deeper than subcutis. The risk of an infection is very low.
Correct answer :
False: Checking pulses in DFU patient is mandatory for all cases. In this case the pulses were present, although not excluding definitely PAD. Only if the wound is not healing in a proper way with good standard of care, the patient must be referred for more profound vascular staging
Correct answer :
True: A holistic approach is needed. It is important to make sure that the patient is not suffering from renal insufficiency and for further management, an optimal treatment of cardiovascular risk factors is essential.
Correct answer :
False: There is no clinical suspicion of deep infection, therefore foot x-ray is not needed at this stage.
Correct answer :
False: A tissue sample is not needed as there is no suspicion of infection and for the same reason no antibiotics need to be started.
What is the overall impression and how the case should be managed?
Correct answer :
False: Although the patient could be referred, if an HCP in primary care can follow the correct standard of care plan , the patient may remain under his/her supervision with weekly medical control and preferably with wound care done by a professional district nurse (or in remote areas by a trained family member).
A careful reevaluation of the wound after 2 weeks is needed: if there is less than 30% reduction of the wound area, a referral to a specialist team is necessary.
Correct answer :
False: The standard of care for all DFUs includes proper debridement (“wound bed preparation”), preferable with sharp debridement (scalpel) and if needed with regular cleansing and using microfiber- pads.
(link to our debridement tool)
Correct answer :
True: the success of treatment of DFU is by taking away the pressure off the ulcer (= off- loading). The golden standard by IWGDF guidance is a Total Contact Cast or a walker that is fixed. In remote areas if this treatment is not available reduction of pressure should be done by felt, foam, bandage shoes, …
(link to IWGDF guidance document of off-loading)
 |  |
Correct answer :
In recent literature it is clear that some modern products can significantly improve healing outcome , but we may not underestimate the importance of off- loading.
(link to TOOL standard of care and IWGDF guidance doc on wound dressings)
What is your final diagnosis and try to classify this DFU according to SINBAD classification
Correct answer :
This DFU is a neuropathic ulcer
-> NON-COMPLICATED DIABETIC FOOT ULCER
Correct answer :
According to SINBAD score we have a score: 2/6
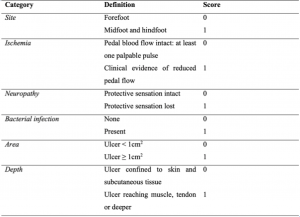
(site: forefoot, ischaemia: no, neuropathy: present, bacterial infection: no, area: >1cm2, depth: not deeper than subcutis)

Wound size after 2 weeks approx. 1,75 cm2.
Reduction of wound area - less than 30%
Refer to your next centre of reference within 2 weeks

Surgical removal of hyperkeratosis
Application of Total Contact Cast
Total wound healing achieved after 2 weeks
Secondary prevention needed = therapeutical shoes and (podiatry)
follow up care is a must

1.Regular follow up by a foot care specialist is mandatory to prevent ulcer recurrence. Therefore, it is advisable to see the foot care specialist every one to three months.
2.Daily self-inspection of the feet and daily foot care is recommended.
3.The patient needs to understand that he should solely wear (therapeutic) footwear appropriate for his feet. Walking barefoot or only with socks has to be avoided.
4.Inform the patient about the need of regular professional foot assessment and treatment.
5.Offer and recommend education to improve knowledge about diabetic foot ulcers and foot care.
6.Offer and recommend education to improve knowledge about diabetes and a healthy lifestyle including cessation of smoking.
1.Such a“ GREEN” case of DFU can be treated according to national standards by HCPs working in primary care, as well as requires a careful follow up and standard of care as prescribed in the TOOL. A reduction of 30% of the wound area is needed at 2 weeks
2.Effective offloading is the mainstay in the treatment of diabetic foot ulcers
3.Each therapy must be frequently critically reviewed. If the therapy is not effective (anymore) one has to question the therapeutic concept and take action to avoid further damage and to optimise the treatment
4.The success will be also determined by the holistic approach to the patient. Loss of vision is critical and needs the correct approach with action to adopt social care