
A 58 year old man, with type 2 diabetes, is referred to a diabetologist with a history of a recent ulcer on the lateral side of the 5th MTPJ.
The duration of DFU was 2 months and was most likely due to trauma from inappopriate footwear.
The patient presented with clinical dyspnea and had a history of acute myocardial infarction 4 years ago.
- To provide an interactive case scenario that takes a clinician through a case study of a complicated DFU
- To reinforce the need for holistic assessment of the patient
- To reinforce the need for incorporating the principles of standards of care in the management of the DFU
- To reinforce the need for early referral to the specialist foot service team or to the Multidisciplinary Foot Team
What factors from patient history would make you concerned?
Correct answer :
No: The foot shows a slowly impairment in the last 5-7 days without fever or systemic signs of sepsis
Correct answer :
Yes: Having such level of pain in a patient with neuropathy partly indicates that the infection of the wound is going into deep tissues
Correct answer :
True: True: We have to find out why the patient was not alarmed. Probably the ulcer was not painful at the start (neuropathy; NO pain= NO alarm). Or the patient never received any education on foot problems, or the patient is in denial or there is no access to care. By reflecting we can intervene in case of new DFU.
Correct answer :
False: the absence of fever does not exclude foot infection as well as further complications such as minor/major amputation
What factors from patient examination would make you concerned?
Correct answer :
Yes: This gives an indication of significant infection.
(link to IDSF/IWGDF guidelines on infection)
Correct answer :
Yes: This indicates a positive “probe to bone” test hence the infection has virtually spread to bone and there is an increased risk of amputation.
(have a link to video on probe to bone test)
Correct answer :
Yes: In the absence of palpable foot pulses, there is a high clinical suspicion of peripheral arterial disease
Correct answer :
No: Although the hypothesis is correct, monofilament test should be carried out during every clinical exam of a patient with DFU.
What investigations would you undertake during the patient’s visit?
Correct answer :
Yes. Heart failure is an independent predictor of amputation and mortality, and can deteriorate the progression of DFU.
Correct answer :
Yes.Dialysis is an independent predictor of amputation and mortality, and can deteriorate the progression of DFU. Furthermore, dialysis is a strong risk factor for peripheral arterial disease.
�
Correct answer :
Yes. History of hypertension, dyslipidemia, and other chronic diseases: in this case the patient suffers from chronic obstructive pulmonary disease (current smoker)
Correct answer :
Yes. Depression is a risk factor for mortality in people presenting with their first DFU and all patients need to be evaluated for depression. This patient is in denial, probably based on depression.
Correct answer :
Yes. This should be standard practice. One should always be aware of the current patient medication list (such as anti-coagulation therapy etc.) especially in case a further intervention is planned.
Correct answer :
Yes. Many patients with DFU have poor diabetes control and poor nutritional status and all this needs to be taken into consideration for appropriate care.
What investigations would you undertake during the patient’s visit?
Correct answer :
True: Body temperature (needs to be taken) often may not be raised and having high blood sugars may be a sign of foot infection
Correct answer :
True: in every patient with DFU, a global staging including assessment of parameters of metabolic control, infection markers (although not raised in every case with clinical infection), kidney function, cardiovascular risk factors (such as LDL, Cholesterol) should be considered.
Correct answer :
False: By global clinical inspection of the foot, the infection is already severe and the wound has been present for 2 months. The chance of having osteomyelitis visible on x-ray is quite high.
Correct answer :
False: Although a tissue sample is needed and could be very useful, one should not delay the initiation of treatment of antibiotics and/ or referral immediately. Taking a tissue sample is very specific and needs the correct skills. (see link with our powerpoint of infection e-footcare).
What is the overall impression and how the case should be managed.
Correct answer :
True: This patient needs to be seen early in a hospital setting where he can have further investigations and limb salvage protocol.
Correct answer :
True: in presence of foot ulcer, the patient should be immediately offloaded and specific shoes for acute phase should be prescribed.
Correct answer :
True: one needs to stress the need for early treatment of infection, including urgent surgical debridement, foot x-ray, review of vascular supply of the foot and management of concomitant co-morbidities. A personal contact will help to make sure that the patient is seenn a.s.a.p. This contact can help you to choose the according antibiotic therapy, adapted to regional resistance. Most of the time AmoxyClav will be the first choice of treatment in this kind of ulcers.
Correct answer :
False. Not at all in this stage. Urgent control of infection should be instituted.Not at all in this stage. Control of infection is the most urgent to go for.
Clinical diagnosis : Infected-ischaemic daibetic foot ulcer in a patient with heart failure
COMPLICATED DIABETIC FOOT ULCER
What is your final diagnosis and try to classify this DFU according to SINBAD classification
Correct answer :
Clinical diagnosis:
Infected neuro-ischaemic diabetic foot ulcer in a patient with heart failure
-> COMPLICATED DIABETIC FOOT ULCER
Correct answer :
According to Sinbad score we have this DFU has a score: 5/6
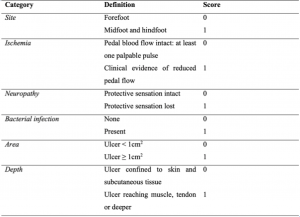
(site: forefoot, ischaemia: yes, neuropathy: present, bacterial infection: yes, area: >1cm2, depth: deeper than subcutis)
The patient was refered to a specialist diabetic foot service after 72 hours
Further examinations:
- Transcutaneous oximetry (TcPO2)=13 mmHg( can’t be done in all settings!)
- Duplex ultrasound: stenosis of superficial femoral artery (SFA), popliteal artery, anterior tibial artery (ATA) and posterior tibial artery (PTA)
- X-Ray: cortical disruption of the proximal phallanx and 5th MT head
- IIID University of Texas Wound Classification
- Grade 5/ 6 (severe) DFU based on SINBAD classification
b) Referral within 4 days due to deterioration of infection (spread from the lateral/dorsal side of the foot to the plantar area) requiring urgent surgical debridement.


 c) Limb salvage protocol
c) Limb salvage protocol
- Antibiotic therapy (initially broad spectrum antibiotics followed by narrow spectrum antibiotics according to results of antibiogram)
- Surgical treatment: sequestrectomy of the 5th MTPJ and partially the 5th MT
- Early Revascularisation (Percutaneous Transluminal Angioplasty of SFA, popliteal, ATA, PTA and pedal artery)
- Offloading
 d) Reconstructive steps
d) Reconstructive steps
- Negative pressure wound therapy
- Dermal substitute
e) Final reconstructive steps:
- Regularly ulcer debridement
- Dressing: TLC-NOSF
- Off-loading
- Management of glycaemia and nutritional status
- Maintenance of antiplatelet and statin therapy
Follow-up in cooperation with First Line


f) Follow-up:
- Secondary prevention by Orthopedic Footwares with perfect fitting and custom made insoles
- Daily personal foot inspection
- Regular follow up by a Specialist Foot care team (every 1-3 month)
Follow-up in cooperation with First Line



1.Patients and HCPs should be trained/educated on the risk of foot ulcers in people with diabetes.
2.Such case of a complicated DFU needs an early fast-track referral to a specialised hospital with a specialist Foot Care Team. ( try to find out such centre in your region!)
3.Early management of infection and ischemia is crucial to reduce amputation and mortality.
4.Co-morbidities such as heart failure and advanced kidney disease could interfere with the prognosis and should be always evaluated for. Nutritional and depression status must not be overlooked.
5.After the acute phase and during the follow-up, a specialist foot care team should cooperate with first line providers to promote healing by using adapted wound dressings and correct off-loading devices, manage concomitant co-morbidities and reduce ulcer recurrence.