 A 38 year old man
A 38 year old man
with type 1 diabetes diagnosed at the age of 12 with HbA1c values higher than 8.5% most of the time
presents to a General Practitioner (GP) with a 48hr history of pain in the left foot after developing a rub from wearing new shoes about a week ago.
- To provide an interactive case scenario that takes a clinician through a case example of a severe complicated DFU
- To reinforce the need for holistic assessment of the patient
- To reinforce the need for incorporating the principles of standard of care in the management of DFU
- To reinforce the need for early referral to the specialist foot service team or to the Multidisciplinary Foot Team
What factors from patient history would make you concerned?
Correct answer :
Yes: The rapid evolution gives an indication that the ulcer is likely to deteriorate very quickly
Correct answer :
Yes: Having such level of pain in a patient with neuropathy partly indicates that the infection or wound is going into deep tissues
Correct answer :
True: The patient is likely to have neuropathy as he would not or did not feel the initial rubbing of the new shoes
Correct answer :
False: the young age does not decrease the risk of complications. On the contrary, he may be at high risk of complications due to the long duration of type 1 diabetes and the need to be more active and mobile
What factors from patient examination would make you concerned?
Correct answer :
Yes: This gives an indication of significant infection and signs of tissue death.
Correct answer :
Yes: This indicates a positive “probe to bone” test hence the infection has spread to the bone and the patient is at high risk of an amputation.
(have a link to video on probe to bone test)
Correct answer :
False: The presence of necrosis or tissue death in such case should override the results of palpable foot pulses as they can also be falsely positive.
Correct answer :
True: It is always important to examine both feet, as having a previous amputations would imply that patient is at high risk of a further amputation.
What factors from patient history would make you concerned?
Correct answer :
Yes: Having systematically high HbA1c values can be an indicator of non – acceptance and denial
Correct answer :
Yes: the outcome of DFU is worse in cases with diabetes related kidney disease
Correct answer :
Yes: Despite his young age, being a smoker together with high LDL and poor diabetes control can contribute to early vascular disease
Correct answer :
Yes: In this situation underlying depression is often overlooked. A holistic approach is needed in such patients as previous history of psycho-social problems can impact on follow up care and patient’s compliance.
What investigations would you undertake during the patient’s visit?
Correct answer :
False: Patients with significant neuropathy may not always mount a systemic response to sepsis as it would be expected by the IDSA criteria. (have a link to IDSA criteria)
Correct answer :
True: Body temperature may not be increased and raised blood sugars may be the only sign of evolving systemic sepsis.
Correct answer :
False: Such a rapidly deteriorating DFU needs to be escalated or actioned upon urgently without delay, or awaiting blood test results.
Correct answer :
False: Although an x-ray could be useful it should not delay the initiation of treatment or the urgent referral to a specialist foot team.
Correct answer :
False: Although a tissue sample is needed and would be useful, it should not delay the initiation of treatment in such rapidly progressing DFU.
What is the overall impression and how the case should be managed.
Correct answer :
True: This patient needs to be seen immediately in a hospital setting where he can have same day investigations with same day results and aggressive treatment. ( <24 Hours!)
Correct answer :
True: the presence of osteomyelitis in the foot also means a risk of fracture to soft inflamed bones and subsequent Charcot deformity.
Correct answer :
True: one needs to stress on the referral the need for urgent treatment of infection, foot x-ray and review of vascular supply to the foot.
Health care providers need to change their attitude to consider a RED DFU case as important as an acute myocardial infarction or Stroke….
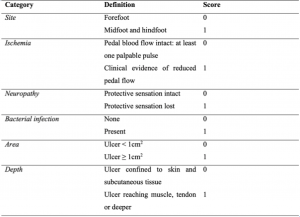
What is your final diagnosis and try to classify this DFU according to SINBAD classification
Correct answer :
This DFU is an infected neuro-ischaemic ulcer
- Severe complicated DFU
Correct answer :
According to Sinbad score, this DFU has a score 5/6.

Urgent surgical draining and debridement of dead and infected tissue.
It is important to have the infection and dead tissue removed surgically and urgently hence the need for urgent referral in such a case.

Initial foot X-ray
Osteomyelitis of the 5th toe and 5th metatarsal. The initial debridement concerns soft and bone tissue.

After the initial surgical debridement of infection one needs to address the ischaemia.
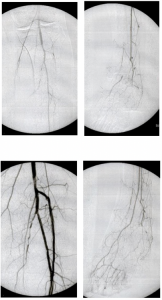
Urgent treatment of ischaemia
The patient presented with a chronic occlusion of the anterior tibial artery (ATA) and posterior tibial artery (PTA). The peroneal artery was the only artery feeding the plantar arch.
After Angioplasty: The anterior tibial artery occlusion was recanalizated with long balloons (2x120 and 3x120): Pedal pulse was present again.
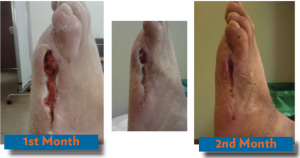
Months 1 and 2: Close follow up, use of negative pressure wound therapy and off-loading.

Months 3 to 4: After 4th toe arthroplasty was performed (conservative surgery), wound closure was achieved, and customised orthotic treatment was initiated

Follow-up:
- A biomechanical study for customised ortothic footwear could be helpful for secondary prevention.
- Daily foot inspection
- Regular follow up with a Specialist Foot care service (monthly)
1.Such case of DFU needs a rapid and fast-track referral to a specialist hospital with a specialist foot care team.
2.Firstly, it is important to treat the severe infection as early as possible and secondly to address the ischaemia. Stop the infection: “Time is tissue”
3.A high grade of ischaemia can be present even in young patients.
4.It is important to have a high index of suspicion of ischaemia due to absence of clinical signs (including absence of rest pain in severe cases according to high prevalence of neuropathy)
5.Speed up the referral pathways to specialist centres if underlying necrotising infections are suspected